

This article is a nice review of where we are (U.S. – and Norwegian – SOF) now in implementing a FWB program. It also gives good background and a simple algorithm of when to pull the trigger to initiate FWB transfusions.
In PFC, we may not have the luxury of confirmed typing and anti-A, anti-B titering, but rapid screening and typing at the point of care, as per the TMEPs protocol, should be adequate for “contingency” use of FWB.
Sean
Huge thanks to the authors of this article for educating our community:
MAJ Andrew D. Fisher, SP USA; MAJ Ethan A. Miles, MC USA; LTC Andrew P. Cap, MC USA; CDR Geir Strandenes, MC; COL Shawn F. Kane, MC USA
Abstract: Recently the Committee on Tactical Combat Casualty Care changed the guidelines on fluid use in hemorrhagic shock. The current strategy for treating hemorrhagic shock is based on early use of components: Packed Red Blood Cells (PRBCs), Fresh Frozen Plasma (FFP) and platelets in a 1:1:1 ratio. We suggest that lack of components to mimic whole blood functionality favors the use of Fresh Whole Blood in managing hemorrhagic shock on the battlefield. We present a safe and practical approach for it’s use at the point of injury in the combat environment called Tactical Damage Control Resuscitation. We describe pre-deployment preparation, assessment of hemorrhagic shock, and collection and transfusion of fresh whole blood at the point of injury. By approaching shock with the goal of replacing what has been lost (blood), it may possible to extend the period of survivability in combat casualties.
Click below to read the entire article:
Tactical Damage Control Resuscitation July 2015
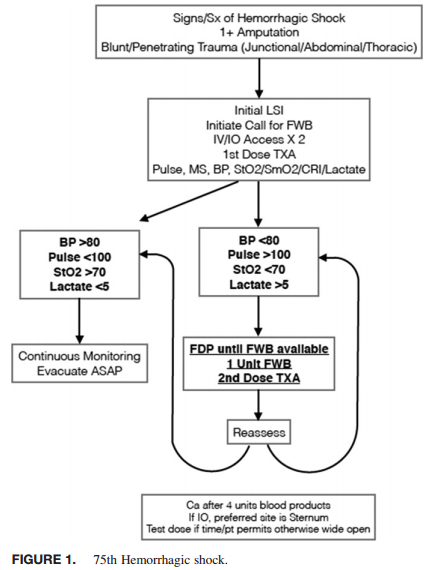
75th Ranger Regiment TDCR Algorithm:

Be sure to check out www.rdcr.org for more blood transfusion resources
Some people have commented that in the algorithm, they don’t have the ability to measure STO2 or point-of-care lactate, therefore they may be unsure or unable to assess when a serious or critical patient may need FWB.
The exact indications for FWB is like the definition of pornography – it’s a bit hard to explain, but you know it when you see it!
Trust your clinical judgement, and resuscitate when indicated. When in doubt, if you have the ability, phone a friend first.
-Sean
…and by phone a friend, I mean initiate a telemedicine consult…
I must say this paper has already inspired some ultrasound fantasies 🙂 A lot of hemodynamic data can be derived from the ultrasound screen… And YES – you are more than capable of learning how to do it!
Great article. I have a few points that may be beneficial from personal experience.
If you think you will get an accurate blood type in the field after you are smoked from a long exfil or something else, your wrong. I recently did my own test where I smoked myself in training treated the patient and tried to type a patient in a confined space, a vehicle and in a secured building in the field. Half of the ABO RH typing i got off the Eldon cards were. The time to type is not at POI. It worth the hassle to have it done before hand, even your partner force. In addition to this a patient who needs blood may not have the IV access or capillary perfusion for an Eldon Card to work. Once again do it early.
I see in the picture the medic has the Y tubing. so he can prep the lines with NS. The newer kits have a single line and there is no need to prep the line. Ounces equal pounds pounds equal weight, that fluid may be better utilized to dilute drugs, antibiotics, etc. If you can, get the single line tubing.
I guess my only question is I know some protocols suggest pushing calcium chloride or calcium gluconate if you are going to give more then 2 units with the whole blood transfusion bags due to the citrate. Can anyone speak to this intelligently?
Based on an article from Up-to-Date (Massive Blood Transfusion)
http://www.uptodate.com/contents/massive-blood-transfusion#H11
& University of Michigan “Massive Transfusion Protocol”
Healthy liver is pretty good at metabolizing citrate… Hypocalcemia is less likely to occur, unless you are infusing more than 1 unit every 5 minutes.
– there is 15 mmol of citrate per 1 liter of transfused whole blood
– max rate of citrate metabolism by a healthy liver is 0.02 mmol/kg (pt weight) per minute – this is your max rate of citrate infusion with transfusion without needing extra calcium
For example, let’s take a 50-kg patient with a healthy liver and no ischemia-induced hepatic dysfunction:
0.02 mmol/kg/min x 50 kg = 1 mmol/min or 60 mmol/hr
This person can receive 60 mmol of citrate per hour without expecting hypocalcemic complications.
With 15 mmol of citrate per 1 L of whole blood, it means that your 50 kg patient can get 4 L in 1 hour without causing citrate toxicity and hypocalcemia. An average unit of blood is 450 mL – so we are talking about 8.9 units of blood.
——
Patients with preexisting liver disease or ischemia-induced hepatic dysfunction have a higher risk of developing hypocalcemic complications in the setting of massive transfusion. In the hospital setting, such patients have their plasma ionized calcium concentration monitored frequently. Calcium is replaced as needed with either calcium chloride or calcium gluconate if ionized hypocalcemia develops.
——
Hope this helps! Other thoughts anyone?
Kevin,
I agree that protocols can differ on when to administer Ca++, we looked at the ISR CPG which recommends Ca++ after four units of FFP. In addition, LTC Andre Cap provided the recommendation in our protocol.
Andrew Fisher
We agree that protocols differ on when to administer Ca++. The ISR CPG on DCR recommends Ca++ after four units of FFP. We also relied on LTC Andre Cap and his expertise in blood research for this protocol. The recommendation was also based off the possibility that a medic or ARFR may only be able to fill 1/2-3/4 of a donor bag due to time or other issues. Thank you for the comments.
Andrew Fisher
Pingback: Podcast Episode 36: ROLO to SOLO: The Logistics of Fresh Whole Blood Transfusion – ProlongedFieldCare.org